Custom Search
|
|
 
|
||
|
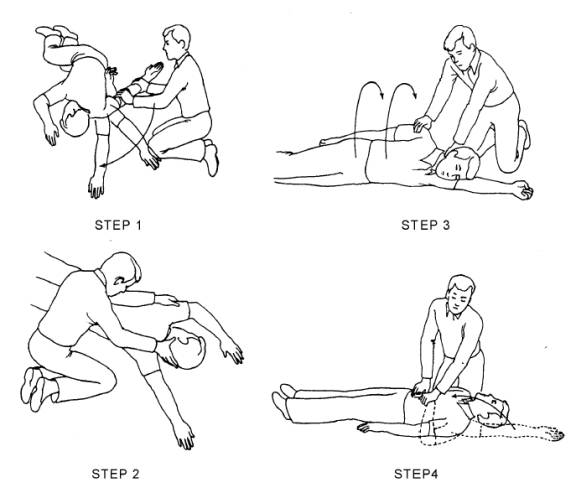
Complete Airway Obstruction Conscious patients will attempt to speak but will be unable to do so. Nor will they be able to cough. Usually, patients will display the universal distress signal for choking by clutching their neck. The unconscious patient with a complete airway obstruction exhibits none of the usual signs of breathing: rise and fall of the chest and air exchange through the nose and/or mouth. A complete blockage is also indicated if a correctly executed attempt to perform artificial ventilation fails to instill air into the lungs. Opening the Airway POSITIONING THE PATIENT.3/4When a patient is unresponsive, you must determine if he is breathing. This assessment requires the patient to be positioned properly with the airway opened. Before repositioning patients, it is imperative that you remember to check them for possible spinal injuries. If there is no time to immobilize these injuries and the airway cannot be opened with the victim in the present position, then great care must be taken when repositioning. The head, neck, and back must be moved as a single unit. To do this, adhere to the following four steps (see figure 4-2). Step 1-Kneel to the side of the victim in line with the victim's shoulders, but far enough away so that the victim's body will not touch yours when it is rolled toward you. Straighten the victim's legs, gently but quickly. Then move the victim's closer arm along the floor until it reaches straight out past the head. Step 2-Support the back of the victim's head with one hand while you reach over with the other hand to grasp under the distant armpit. Step 3-Pull the patient toward you while at the same time keeping the head and neck in a natural straight line with the back. Resting the head on the extended arm will help you in this critical task. Step 4-Roll the patient onto his back and reposition the extended arm. Once the patient is supine with the arms alongside the body, you should position yourself at the patient's side. By positioning yourself at the patient's side, you can more easily assess whether the patient is breathing. If the patient is not breathing, you are already positioned to perform artificial respirations (also referred to as rescue breathing) and chest com- pressions. Either one of two maneuvers-the head tilt-chin lift maneuver or the jaw-thrust maneuver-may be used to open an obstructed airway. When performing these maneuvers, you may discover foreign material or vomitus in the mouth that needs to be removed. Do not spend very much time to perform this task. Liquids or semiliquids should be wiped out with the index and middle finger covered by a piece of cloth. Solid material should be extracted with a hooked index finger. HEAD TILT-CHIN LIFT MANEUVER.-The head tilt-chin lift maneuver is the primary method used to open the airway. To perform the head tilt-chin lift maneuver, place one of your hands on the patient's forehead and apply gentle, firm, backward pressure using the palm of your hand. Place the fingers of the other hand under the bony part of the chin. Lift the chin forward and support the jaw, helping to tilt the head back. See figure 4-3. This maneuver will lift the patient's tongue away from the back of the throat and provide an adequate airway. PRECAUTIONS: When performing the head tilt-chin lift maneuver, do not press too deeply into the soft tissue under the chin. Undue pressure in this location may obstruct the airway. In addition, make sure the mouth is kept open so exhalation and inhalation are not hindered. JAW-THRUST MANEUVER.-The jaw-thrust maneuver is considered an alternate method for opening the airway. This maneuver is accomplished by kneeling near the top of the victim's head, grasping the angles of the patient's lower jaw, and lifting with both hands, one on each side. This will displace the mandible (jawbone) forward while tilting the head backward. Figure 4-4 illustrates the jaw-thrust maneuver. If the lips close, retract the lower lip with your thumb. If mouth-to-mouth breathing is necessary, close the nostrils by placing your cheek tightly against them. NOTE: The jaw-trust technique without head tilt is considered the safest approach to opening the airway of patients with suspected neck injuries because it usually can be done without extending the neck. Figure 4-2.-The four steps to reposition the victims of spinal injuries.
Figure 4-4.-Jaw-thrust maneuver. |
 
|
|
|
||