Custom Search
|
|
 
|
||
|
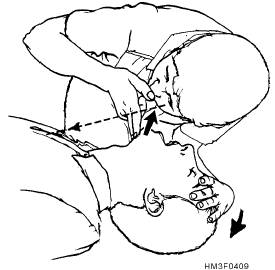
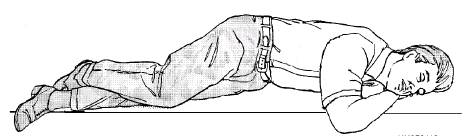
BREATHING The second aspect of basic life support is to restore breathing in cases of respiratory arrest. Failure of the breathing mechanism may be caused by various factors. They include complete airway obstruction, insufficient oxygen in the air, inability of the blood to carry oxygen (e.g., carbon monoxide poisoning), paralysis of the breathing center of the brain, and external compression of the body. Respiratory arrest is usually but not always immediately accompanied by cardiac arrest. Periodic checks of the carotid pulse must be made, and you must be prepared to start cardiopulmonary resuscitation (CPR). Signs of respiratory arrest are an absence of respiratory effort, a lack of detectable air movement through the nose or mouth, unconsciousness, and a cyanotic discoloration of the lips and nail beds. Determining Breathlessness Step 1 3/4 Place your ear over the patient's mouth and nose, while maintaining an open airway. Step 2 3/4 While observing the patient's chest, listen for air escaping during exhalation, and Recovery Position To place a patient in the recovery position, roll the patient onto his side so that the head, shoulders, and torso move simultaneously without twisting. If the patient has sustained trauma or trauma is suspected, the patient should NOT be moved. Artificial Ventilation Techniques of artificial ventilation include mouth-to-mouth, mouth-to-nose, mouth-to-stoma, and mouth-to-mask. These techniques as they apply to adult patients are discussed in the following sections. MOUTH-TO-MOUTH.-Artificial ventilation with the mouth-to-mouth technique is a quick, style="mso-spacerun: yes"> effective way to provide oxygen to the patient. The exhaled air contains enough oxygen to supply the patient's needs. To perform mouth-to-mouth ventilation, the airway must be open. To open the airway, perform the head tilt-chin lift or jaw-thrust maneuver. If there is no spontaneous breathing, start artificial ventilation by pinching the nose closed with your thumb and index
Figure 4-9.-Determining breathlessness. finger. Take a deep breath and seat your lips around the patient's mouth (creating an airtight seal), and give two slow ventilations (1 1/2 to 2 seconds per breath). See figure 4-11. Allow enough time for the lungs to deflate between ventilations. If the patient still does not respond, continue mouth-to-mouth ventilations at the rate of 10 to 12 ventilations per minute or one breath every 5 seconds. Periodically, check the pupils for reaction to light; constriction is a sign of adequate oxygenation. NOTE: When performing artificial ventilation and the lungs cannot be inflated adequately, repeat head tilt-chin lift or jaw-thrust maneuver, and again attempt ventilation. If the lungs still do not inflate adequately, assume the airway is obstructed by a foreign object. MOUTH-TO-NOSE.-Mouth-to-nose ventilation is effective when the patient's mouth cannot be opened (lockjaw), extensive facial or dental injuries occur, or an airtight seal of the mouth cannot be achieved. Figure 4-12 shows an example of this procedure. To administer this technique, tilt the head back with one hand on the patient's forehead and use the other hand to lift the jaw (as in the head tilt-chin lift maneuver). Close the victim's mouth. Take a deep breath, seal your lips around the patient's nose, and give two ventilations. Allow the victim's lungs to deflate passively after each ventilation. If the victim does not respond, then you must fully inflate the lungs at the rate of 10 to 12 ventilations per minute or one breath every 5 seconds until the victim can breathe spontaneously. MOUTH-TO-STOMA.-A casualty who has had surgery to remove part of the windpipe will breathe through an opening in the front of the neck called a stoma. Cover the casualty's mouth with your hand, take a deep breath, and seal your mouth over the stoma. Breathe slowly, using the procedures for mouth-to-mouth breathing. Do not tilt the head back. (In some situations, a person may breathe through the stoma as well as his nose and mouth. If the casualty's chest does not rise, cover his mouth and nose, and continue breathing through the stoma.) MOUTH-TO-MASK.-The mouth-to-mask breathing device includes a transparent mask with a one-way valve mouth piece. The one-way valve directs the rescuer's breath into the patient's airway while diverting the patients's exhaled air away from the rescuer. Some devices have an oxygen adaptor that permits the administration of supplemental oxygen. Figure 4-10.-A patient in the recovery position.
Step 1-Place the mask around the patient's mouth and nose, using the bridge of the nose as a guide for correct position. Proper positioning of the mask is critical because gaps between the mask and the face will result in air leakage. Step 2--Seal the mask by placing the heel and thumb of each hand along the border of the mask and compressing firmly to provide a tight seal around the margin of the mask. Step 3--Place your remaining fingers along the bony margin of the jaw and lift the jaw while performing a head tilt. Step 4--Give breaths in the same sequence and at the same rate as in mouth-to-mouth resuscitation; observe the chest for expansion. |
||
|
||