Custom Search
|
|
 
|
||
|
BREATHING AIDS
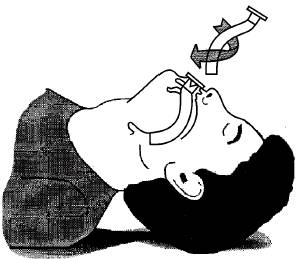
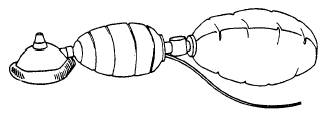
LEARNING OBJECTIVE: Recognize breathing aids and their uses. As a Hospital Corpsman, you should become familiar with the breathing aids that may be available to help you maintain an open airway and to restore breathing in emergency situations. Breathing aids include oxygen, artificial airways, bag-valve mask ventilator, pocket face mask, and suction devices. USE OF OXYGEN (O2) When available, oxygen should be administered, as described below, to cardiac arrest patients and to self-ventilating patients who are unable to inhale enough oxygen to prevent hypoxia (oxygen deficiency). Hypoxia is characterized by tachycardia, nervousness, irritability, and finally cyanosis. It develops in a wide range of situations, including poisoning, shock, crushing chest injuries, cerebrospinal accidents, and heart attacks. Oxygen must never be used near open flames since it supports burning. Oxygen cylinders must be handled carefully since they are potentially lethal missiles if punctured or broken. ARTIFICIAL AIRWAYS Oropharyngeal Airway One method of insertion is to depress the tongue with a tongue blade and slide the airway in. Another method is to insert the airway upside down into the victim's mouth; then rotate it 180 as it slides into the pharynx (fig. 4-20). Nasopharyngeal Airway BAG-VALVE MASK VENTILATOR Various types of bag-valve-mask systems that come in both adult and pediatric sizes are in use in the Navy. Essentially, they consist of a self-filling ventilation bag, an oxygen reservoir, plastic face masks of various sizes, and tubing for connecting to an oxygen supply.
Figure 4-20.-The rotation method of inserting an
oropharyngeal airway.
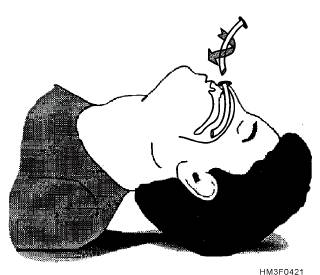
Figure 4-21.-Proper insertion of a nasopharyngeal airway.
The bag-valve mask ventilator is difficult to use unless the user has had sufficient practice with it. It must not be used by inexperienced individuals. The system can be hard to clean and reassemble properly; the bagging hand can tire easily; and an airtight seal at the face is hard to maintain, especially if a single rescuer must also keep the airway open. In addition, the amount of air delivered to the victim is limited to the volume that the hand can displace from the bag (approximately 1 liter per compression). Procedures for Operating the Bag-Valve Mask Ventilator To use the bag-valve mask ventilator, hook the bag up to an oxygen supply and adjust the flow in the range of 10 to 15 liters per minute, depending on the desired concentration (15 liters per minute will deliver an oxygen concentration of 90 percent). After opening the airway or inserting an oropharyngeal airway, place the mask over the face and hold it firmly in position with the index finger and thumb, while keeping the jaw tilted upward with the remaining fingers (fig. 4-23). Use the other hand to compress the bag once every 5 seconds. Observe the chest for expansion. If none is observed, the face mask seal may not be airtight, the airway may be blocked, or some component of the bag-valve mask ventilator may be malfunctioning. |
 
|
|
|
||