

Custom Search
|
|
 
|
||
|
INGESTED POISONS Ingested poisons are those poisons which have been consumed, whether accidentally or intentionally, by the victim. Ingestion is the most common route of exposure to toxic materials in the home. The local actions of an ingested poison can have irritant, acidic (corrosive), or basic (caustic) effects at the site of contact. Table 5-1.-Commonly Encountered Toxidromes Ingested substances can be absorbed into the body and transported to a distant site with systemic action(s). In such situations, the poisonous substance may cause few effects-or even no effect-at the site of contact or absorption, but it may have severe systemic effects. Ingestion of substances that do not produce local effects can be divided into two types: nontoxic substances (latex paint, dirt, silica gel, spider plant), and potentially toxic substances (poisonous fish, medications, heavy metals
(lead, mercury), pesticides, and
personal care products). The toxicity range of absorbed poisons extends from essentially non-toxic to extremely toxic (remember Paracelsus' "dose"). Ingestion of substances with a low order of toxicity may result in the production of only minor systemic effects (nausea, vomiting, diarrhea), effects that are mild, self-limiting, and do not require significant medical intervention. NOTE: Do not induce unnecessary vomiting to discourage a patient from repeating a voluntary ingestion again. Noncorrosives First aid for most forms of noncorrosive poisoning centers on quickly emptying the stomach of the irritating substance. The following steps are suggested: 1. Maintain an open airway. Be prepared to give artificial ventilation. 2. Dilute the poison by having the conscious victim drink one to two glasses of water or milk. 3. Empty the stomach using emetic, gastric lavage, adsorbent, and/or cathartic. a. Giving an emetic is a preferred method for yes">emptying the contents of the stomach.
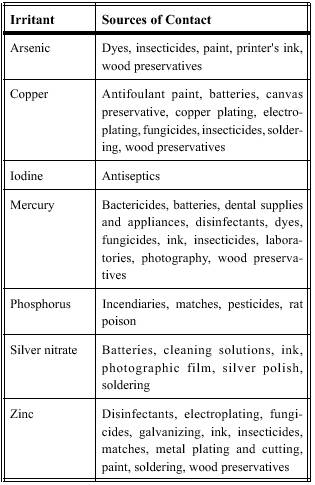
Table 5-2.-Common Stomach Irritants and Possible Sources
of Contact b. Trained personnel may use gastric lavage by itself or after two doses of Ipecac syrup has failed to induce vomiting. After passing a large-caliber nasogastric tube, aspirate the stomach contents. Next, instill 100 ml of normal saline into the stomach, then aspirate it out again. Continue this flushing cycle until the returning fluid is clear. Gastric lavage is preferred when the victim is unconscious or-as in the case of strychnine poisoning-is subject to seizures. c. Activated charcoal (AC) adsorbs many substances in the gut and prevents absorption into the body. After the substance is adsorbed to the AC, the bound substance moves through the gut and is eliminated with the production of a charcoal-black bowel movement. AC may be administered after emesis or lavage, or it may be used alone. d. A cathartic (magnesium sulfate or sorbitol) may be used to "speed" the movement of the bound substance and minimize absorption. 4. Collect the vomitus for laboratory analysis. 6. Transport the victim to a definitive care facility if symptoms persist. |
 
|
|
|
||















 style="mso-spacerun: yes">
style="mso-spacerun: yes">