Custom Search
|
|
 
|
||
|
LYMPHATIC CONSTRICTION
INSTRUCTIONS
An appropriate lymphatic constriction device is a blood pressure cuff, inflated to the diastolic blood pressure (so the blood can be felt flowing past the cuff). Other devices may be used, but IT IS IMPORTANT THAT BLOOD CIRCULA- TION TO THE BITE AREA BE MAINTAINED. Constriction should be fully released every 30 minutes for 15 seconds. If the constriction pressure cannot be carefully controlled, THE MAXIMUMTOTALTIME OFUSE OFTHE CONSTRICTION DEVICE IS 2 HOURS. (Thus, three 15-second breaks, and the fourth time the cuff, belt, or band remains OFF.) NOTE: If you use a blood pressure cuff (or
device that you KNOW is not constricting
more than an Ace 7 bandage on a sprain),
you may continue to apply constriction
until the patient reaches a hospital. If possible, antivenom specific to the snake should be used. Otherwise, a "polyspecific" antivenom may be used. READ THE PACKAGE INSERT OF THE ANTIVENOM FOR VALUABLE INFORMATION. Epinephrine and diphenhydramine must be available, as allergic reactions (including anaphylaxis) to antivenom have occurred (they are often prepared from horse serum, which some people are allergic to). Antivenom is diluted (for example, 1:10) and given at 5 ml/minute IV, and the dose is based on stopping the progression of signs and symptoms, not the victim's body weight (the children's dose is the same as the adult dose). For neurotoxic snakebites, if there is no improvement in 30 minutes, the dose should be repeated. For Viperidae (which can cause bleeding disorders), spontaneous bleeding should stop after sufficient antivenom is given; continue giving antivenom until bleeding stops and progression of swelling is retarded. Because you may need to administer antivenom a number of times, one vial may not be enough to treat a patient. Antivenom is available via PCCs and hospitals. It may also be available at zoos and embassies. The "Don'ts" of Snakebite Treatment.-The following are the "don'ts" when it comes to treatment of snakebite. DO NOT use any ice or cooling on the bite. DO NOT use electric shock. DO NOT give victim alcohol or narcotics. Further information may be obtained on an emergent basis from a PCC or from Arizona Poison Control, (520) 626-6016. Bites, Stings, and Punctures from Sea Animals JELLYFISH INJURIES.-Other sea animals yes"> inflict injury by means of stinging cells located in tentacles. This group includes the jellyfish and the Portuguese man-of-war (fig. 5-5). The tentacles (which may be impossible to see, even in relatively clear water) release poison or tiny stingers through which poison is injected into the victim. Jellyfish stings may cause symptoms ranging from minor irritation (pain and itching) to death. Contact with the tentacles produces burning pain, a rash with small hemorrhage in the skin, and, on occasion, shock, muscular cramping, nausea, vomiting, and respiratory and cardiac distress. Treatment for minor jellyfish injuries consists of pouring sea water over the injured area and then removing the tentacles with a towel or gloves. Next, pour rubbing alcohol, formalin, vinegar, meat tenderizer, or diluted ammonia over the affected area to neutralize any remaining nematocysts (minute stinging structures). Finally, cover the area with any dry powder (to which the last nematocysts will Figure 5-5.-Jellyfish and Portuguese Man-of-war. Some jellyfish (notably, the Portuguese man-of-war, the box jellyfish, and certain jellyfish from northeastern Australia) may cause serious injuries and even have the potential to be lethal. In cases where the kind of jellyfish that caused the sting is either unknown or is known to have been from a box jellyfish or Portuguese man-of-war, the injury should be treated as a serious one, regardless of initial symptoms. The following steps should be taken in the case of serious jellyfish stings. 1. Retrieve the victim from the water if necessary. 3. Pour vinegar liberally (2 liters) over the sting area for at least 30 seconds to inactivate stinging cells that may remain. 4. Remove any remaining tentacles carefully. (Excessive manipulation may cause rupture of nematocysts and further poison release.) Carefully (and gently) use a towel if necessary, or use a dull knife edge (as described above to remove arthropod stingers). 5. Apply a compression bandage to stings covering more than half of one limb or causing altered consciousness. 6. Start an IV. 8. Transport the patient to a hospital as quickly as possible. 9. Opiate analgesics (morphine or meperidine) may be necessary for pain relief. "SPINE" INJURIES.-Spiny fish, stingrays,
urchins, and cone shells inject their venom by
puncturing with spines (fig. 5-6). General
signs and symptoms include swelling,
nausea, vomiting, generalized cramps,
diarrhea, muscular paralysis, and shock.
General emergency care consists of prompt
flushing with cold sea water to remove the venom and
to constrict hemorrhaging blood vessels.
Next, debride the wound of any
remaining pieces of the spine's
venom-containing integumentary sheath. Soak
the wound area in very hot water (110F/43 C) for 30
to 60 minutes to neutralize the venom.
Finally, In the case of contact with stonefish, scorpionfish, zebra, or lionfish, immerse the wound in very hot water for a minimum of 30 minutes until the pain is decreased. Inject emetine hydrochloride directly into the wound within 30 minutes, and provide meperidine (or other opiate) for pain. Monitor the victim's vital signs closely. Obtain antivenom (from local zoos or aquariums) for all serious cases. SEASNAKE INJURIES.-Sea snakes are found in the warm water areas of the Pacific and Indian Oceans. Their venom is VERY poisonous, but their fangs are only 1/4 inch long. The first aid outlined for land snakes also applies to sea snakes.
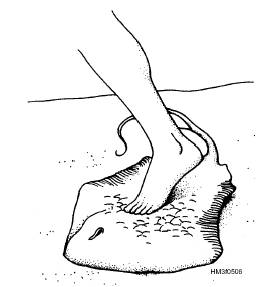
Figure 5-6.-Stingray sting.
|
 
|
|
|
||