Custom Search
|
|
 
|
||
|
REPORTING THE COUNT.-When you have
calculated the differential count, the report is given
according to either the Schilling
classification or filament and
nonfilament classification methods. We
will be covering the Schilling classification, since
it is the simplest and most popular method.
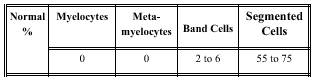
The Schilling Classification.-The Schilling classification was established when Victor Schilling, a German hematologist, noticed that in many diseases there is an increase in the percentage of immature neutrophils. The blood chart he developed reported the percentages of the different neutrophilic cell types and (in part) was arranged in the following manner: Note that the immature cells are on the left side of the chart. If percentages of immature cell increased, Schilling referred it as a "shift to the left." When the shift to the left was accompanied by a low white cell count, Schilling called it a "degenerative shift to the left." A degenerative shift to the left is seen in such diseases as typhoid fever. This shift is caused by a depression of the cell factories in the bone marrow. When the shift to the left is accompanied by a high white cell count, it is called a "regenerative shift to the left." A regenerative shift to the left is seen in such diseases as pneumonia. This shift is caused by a stimulus of the cell factories in the bone marrow. A "shift to the right" implies an increase in hypersegmented neutrophils. It may be seen in pernicious anemia, an anemia caused by the malabsorption of vitamin B12. The Schilling classification for an adult differen- tial white cell count is provided below in table 7-2. NOTE: Normal values for differential counts vary with the age of the patient. For example, children's blood normally contains 0% to 2% basophils, 0% to 5% eosinophils, 25% to 75% neutrophils, 30% to 70% lymphocytes, and 0% to 8% monocytes. Normal values may also be adjusted by hospitals that have evaluated the normal differential value for their local population. General Interpretations of Leukocyte Changes.-Together, the total white cell count and differential count aid physicians in interpreting the severity of infections. Some general interpretations of leukocyte changes are as follows: Leukocytosis with an increase in the percentage of neutrophils indicates a severe infection with a
Table 7-2.-Schilling Classification of the Differential White A falling white cell count with the number and maturity of neutrophils
progressing toward normal indicates
recovery. The percentage of eosinophils, lymphocytes, and monocytes generally
decreases in acute infections. Eosinophils increase in parasitic infections and allergic conditions. |
||
|
||