Custom Search
|
|
 
|
||
|
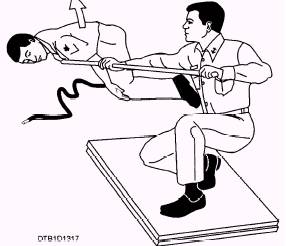
TREAT TO PREVENT INFECTION.\Cover the entire burned area with a sterile dressing. Do not put ointments, antiseptics, or other medications on a burn. These will interfere with later treatment. To prevent infection of the burn, you must observe the following precautions: Never allow any unsterile objects or material to come into contact with the burn. (However, in an emergency situation when no sterile dressing is available, you may cover the burn with a clean sheet or an unused plastic bag.) Never use rough textured materials like blankets to cover the burn. Never attempt to break blisters. Never attempt to remove shreds of tissue or charred clothing from the burn. For thermal burns of the eye, make sure that the casualty does not rub the eyes. Cover each eye with a small, moist, thick compress. Fasten the compress in place with a bandage. Treat the casualty for shock. To treat for shock, maintain the casualty's body heat, but do not allow the casualty to become overheated. If the casualty is in severe pain, you may administer morphine, but only under the mass casualty conditions discussed earlier. A seriously burned casualty has an overwhelming need for liquids. If the casualty is conscious, has no internal injuries, and is not vomiting, prepare a weak solution of salt (1 teaspoon) and baking soda (1/2 teaspoon) in a quart of warm water. Allow the casualty to sip slowly. Chemical Burns.\Corrosive chemicals that come in contact with body tissues may cause chemical burns. To treat acasualty with a serious chemical burn, take the following steps: 1. Immediately flush the burned area with large amounts of water. Pour water over the area; use a hose or shower if one is available. Do not apply water too forcefully, because this could further damage the burned tissue. While the area is being flushed, remove the casualty's clothing, including the shoes and socks. Keep flushing the area until all traces of the chemical have been removed. 2. Gently pat the burned area with sterile gauze. Do not rub the area with the gauze. Be careful not to break the skin or open any blisters. 3. Prevent infection by covering the entire burned area with a sterile dressing, just as you would for a thermal burn. 4. Treat for shock, just as you would for a thermal burn. For chemical burns of the eye, make sure that the casualty does not rub the eyes. Immediately flush the eyes with large quantities of fresh, clean water. Have the casualty lie down with the head turned slightly to one side. To flush the eye, pour water into the inside corner of the eye and let it flow across the eyeball to the outside corner. The water must not be poured with any greater force than is necessary to sustain the flow across the eyeball. Because of the intense pain, the casualty may be unable to open the eyes. If this occurs, you must hold the eyelids open so that the water can flow across the eyeball. After irrigating the eyes, loosely cover them with a sterile dressing. Treat the casualty for shock. Electrical Burns.\Electrical burns are more serious than they first appear. The entrance wound may be small, but as electricity penetrates the skin, it burns a large area below the surface. Usually there are two external burn areas: one where the current enters the body and another where it leaves. Before administering emergency treatment, remove the casualty from the electrical source. If power equipment is involved, shut it off or disconnect it immediately. When rescuing a casualty who is in direct contact with a power line, stand on a well-insulated object, and use a dry rope or a wooden pole to either push or pull the wire away from the casualty, or the casualty away from the wire (fig. 13-17). Do not touch the casualty until this is done or you, too, will become a casualty. Electrical burns are often accompanied by respiratory failure and cardiac arrest, which are of more immediate danger to the casualty than the burn
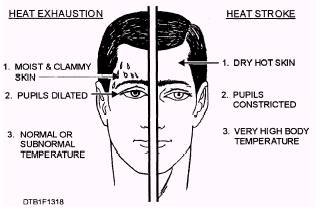
Figure 13-17.\Pushing a casualty away from a power line. itself. Start cardiopulmonary resuscitation (CPR) (explained in Dental Technician, Volume 2, NAVEDTRA 12573, chapter 9) immediately and continue until the casualty regains a normal heartbeat and breathing pattern. Finally, lightly cover the site of the burn with a preferably dry sterile dressing, treat for shock, and transport the casualty to a medical facility. HEAT EXPOSURE INJURIES.\Excessive heat affects the body in a variety of ways. When a person exercises in a hot environment, heat builds up inside the body. The body automatically reacts to get rid of this heat through the sweating mechanism. If the body loses large amounts of water and salt from sweating, heat cramps and heat exhaustion are likely to follow. When the body becomes overheated and cannot eliminate the excessive heat, heat stroke will result. Heat Cramps.\Heat cramps usually affect people who work in hot environments or who engage in strenuous exercise without acclimatization and proper training. Excessive sweating may result in painful heat cramps in the muscles of the abdomen, legs, and arms. Heat cramps may also result from drinking ice water or other cold drinks either too quickly or in too large a quantity after exercise. Muscle cramps are often an early sign of approaching heat exhaustion. Muscle spasms or heat cramps usually last only a few minutes and disappear spontaneously. To provide emergency treatment for heat cramps, move the casualty to a cool place. Heat cramps are caused by loss of salt and water, so give the casualty plenty of water to drink, adding about 1 teaspoon of salt to a quart of water. Apply manual pressure to the cramped muscle, or gently massage it to relieve the spasm. If the heat cramps do not pass, or if they become more severe, other symptoms may follow. The casualty should be treated as a heat exhaustion casualty and then transferred to a medical facility for further treatment. Heat Exhaustion.\Heat exhaustion is the most common condition resulting from exposure to hot environments. Heat exhaustion is not easily diagnosed because it can be a combination of several factors. Because of these factors, the signs and symptoms may vary. As a general rule, heat exhaustion will involve a serious disturbance of blood flow to the brain, heart, and lungs. This may cause the casualty to experience weakness, fatigue, headache, loss of appetite, and nausea. The person may faint, but will probably regain consciousness when the head is lowered to improve the blood supply to the brain. The casualty will appear ashen gray, the skin will be cold, moist, clammy, and the pupils of the eyes may be dilated (enlarged). Vital signs are usually normal but the casualty may have a weak pulse, together with rapid, shallow breathing. The body temperature may be below normal. Treat the casualty as if the patient were in shock. Move the person to a cool or air-conditioned area. Loosen the clothing; apply cool wet cloths to the head, neck, groin, and ankles; and fan the casualty. Do not allow the person to become chilled. If they become chilled, cover with a light blanket and move to a warmer area. If the casualty is conscious, give a solution of 1 teaspoon of salt mixed in a quart of cool water. If the person vomits, do not give any more fluids. Transport the casualty to a medical facility as soon as possible. Heat Stroke.\Sunstroke is more accurately called heat stroke because a person need not be exposed to the sun for the condition to develop. Heat stroke is a less common but far more serious condition than heat exhaustion because it carries a 20 percent mortality rate. The most important feature of heat stroke is the extremely high body temperature (105F or 41C) or higher. In heat stroke, the casualty's sweating mechanism breaks down and cannot eliminate excess body heat. If the body temperature rises too high, the brain, kidneys, and liver may be permanently damaged. Sometimes the casualty may have preliminary symptoms such as headache, nausea, dizziness, or weakness. Breathing will be deep and rapid at first; later it will be shallow and almost absent. Usually the casualty will be flushed, very dry, and very hot. Pupils will be constricted (pinpointed) and the pulse will be fast and strong. Compare heat stroke symptoms with those of heat exhaustion. (See figure 13-18.)
Figure 13-18.\Symptoms of heat exhaustion and heat stroke. When providing emergency treatment for heat stroke, keep in mind that if the casualty remains overheated, the more likely he/she will suffer irreversible body damage or death. Your main objective is to get the body temperature down as quickly as possible. Move the casualty to the coolest possible place, and remove as much clothing as possible. Body heat can be reduced quickly by immersing the casualty in a cold water bath. If that is not possible, give the casualty a sponge bath by applying wet, cold towels to the entire body. Or you can expose him/her to a fan or air conditioner. If cold packs are available, place them under the arms, around the neck, at the ankles, and in the groin. If the casualty is conscious, give him/her cool water to drink. Do not give any hot drinks or stimulants. Because of the seriousness of heat stroke, it is important to get the casualty to a medical facility as soon as possible. Continue the cooling measures during transportation. |
 
|
|
|
||
|
|
Integrated Publishing, Inc. - A (SDVOSB) Service Disabled Veteran Owned Small Business
|