| Tweet |

Custom Search
|
|
 
|
||
|
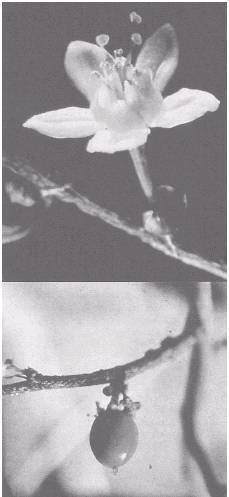
Meprobamate Meprobamate first synthesized in 1950, introduced the era of mild or "minor" tranquilizers. In the United States today more than 200 tons of meprobamate are distributed annually under its generic name as well as under brand names such as Miltown, Equanil, Kesso-Bamate, and SK-Bamate. Meprobamate is prescribed primarily for the relief of anxiety, tension, and associated muscle spasms. Its onset and duration of action are like those of the intermediate-acting barbiturates. It differs from them in that it is a muscle relaxant, does not produce sleep at therapeutic doses, and is relatively less toxic. Excessive use, however, can result in psychological and physical dependence. Mebutamate (Dormate), a drug similar to meprobamate in its chemical makeup and effects, is also regulated under the FCSA. Benzodiazepines These substances are marketed as mild or minor tranquilizers, sedatives, hypnotics, or anticonvulsants. Their margin of safety is greater than that of other depressants. Fifteen members of the group are currently marketed in the United States. The are alprazolm (Xanax), chlordiazepoxide (Librium), clonazepam (Klonopin), clorazepate (Tranxene, Azene), diazepam (Valium), estazolm (Prosom), flurazepam (Dalmane), halazepam, Iorazepam (Ativan), midazolam, oxazepam (Serax), prazepam (Verstran), quazepam (Doral), temazepam (Restoril), and triazolam (Halciun). Prolong use of therapeutic or excessive doses may result in physical and psychological dependence. These drugs are also used by people in methadone maintenance programs in combination with narcotics such as methadone to obtain a "high." STIMULANTS The two most prevalent stimulants are nicotine in tobacco products, and caffeine, the active ingredient of coffee, tea, and some beverages sold in every supermarket. These two stimulants, even when used in moderation, have a dependence-producing potential. These stimulants tend to relieve fatigue and increase alertness, and they are an accepted part of our culture. There are, however, more potent stimulants that, because of their dependence-producing potential, are under the regulatory control of the FCSA. Some of these controlled stimulants, such as amphetamine, methamphetamine, methylphenidate, and cocaine, are available on prescription for medical purposes. They are also clandestinely manufactured in vast quantities for distribution on the illicit market. Users tend to rely on stimulants to feel stronger, more decisive, and self-possessed. Because of the cumulative effects of the drugs, chronic users often follow a pattern of taking uppers in the morning and downers such as alcohol or sleeping pills at night. Such chemical manipulation interferes with normal body processes and can lead to mental and physical illness. Young people who resort to stimulants for their euphoric effects consume large doses sporadically, over weekends or at night, often going on to experiment with other drugs of abuse. In contrast, some people go on a drug binge lasting from 2 to 8 days, administering drugs over and over without sleeping or eating. The consumption of stimulants may result in a temporary sense of exhilaration, superabundant energy, hyperactivity, extended wakefulness, and a loss of appetite. It may also induce irritability, anxiety, and apprehension. These effects are greatly intensified with administration by intravenous injection, which may produce a sudden sensation known as a "flash" or "rush." The protracted use of stimulants is followed, however, by a period of depression known as "crashing" that is invariably described as unpleasant. Since the depression can be easily counteracted by an injection of stimulant, this abuse pattern becomes increasingly difficult to break. Heavy users may inject themselves every few hours, a process sometimes continued to the point of delirium, psychosis, or physical exhaustion. Tolerance develops rapidly to both the euphoric and appetite suppressant effects. If withdrawn from stimulants, chronic high-dose users exhibit profound depression, apathy, fatigue, and disturbed sleep for up to 20 hours a day. The immediate withdrawal syndrome may last for several days. There may also be a lingering impairment of perception and thought processes. Anxiety, an incapacitating tenseness, and suicidal tendencies may persist for weeks or months, Many experts now interpret these symptoms as indicating that stimulant drugs are capable of producing physical dependence. Whether the withdrawal syndrome is physical or psychological is, in this instance, academic since the stimulants are recognized as among the most potent agents of reward and reinforcement that underlie the problem of dependence. Cocaine The most potent stimulant of natural origin, cocaine is extracted from the leaves of the coca plant (erythroxylon coca). (See figs. 7-8 and 7-9.) Illicit cocaine is distributed as a white crystalline powder (fig. 7-10), often adulterated to about half its
Figure 7-8.-Coca flower and bean. volume by a variety of other ingredients, the most common of which are sugars such as lactose, inositol, mannitol, and local anesthetics such as lidocaine. Since the cost of illicit cocaine is high, them is a tendency to adulterate the product at each level of distribution. The drug is most commonly administered by being "snorted" through the nasal passages. Symptoms of repeated use in this manner may
Figure 7-9.-Coca leaf. resemble the congested nose of a common cold and may cause damage to the septum of the nose. Less commonly, for heightened effect, the drug is injected directly into the bloodstream. Cocaine may also be smoked by free basing. Free basing is a process using a solvent to convert the cocaine to a base. The solvent itself is dangerous and the smoking can result in overdose. This is because the drug immediately enters the bloodstream and the user cannot control dosage. Unlike such drugs as LSD and heroin, cocaine is popularly accepted as a recreational drug, facilitating social interaction. It is erroneously said to be relatively safe from undesirable side effects. Because of the intensity of its pleasurable effects, cocaine has the potential for extraordinary psychic dependency, which is all the more deceptive in view of its reputation as the recreational drug of choice. Tolerance seldom develops; however, recurrent users may resort to larger doses at shorter intervals until their lives are largely committed to their habituation. Anxiety, restlessness, and extreme
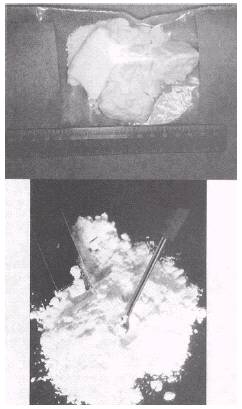
Figure 7-10.-Cocaine. irritability may indicate the onset of a toxic psychosis similar to paranoid schizophrenia. Tactile hallucinations so afflict some chronic users that they injure themselves in attempting to remove imaginary insects from under the skin. Others are persecuted by the fear of being watched and followed. Excessive doses of cocaine may cause seizures and death from respiratory failure. Some drug abusers use cocaine with other drugs such as morphine or heroin, Combination shots of cocaine and heroin, cocaine and morphine, or all three are called "speedballs."
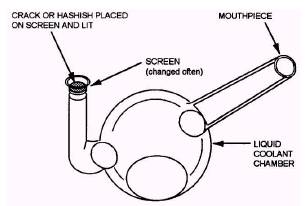
Figure 7-11.-Crack pipe (glass). |
 
|
|
|
||