Custom Search
|
|
 
|
||
|
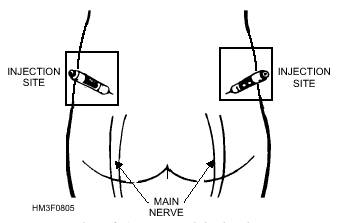
CHEMICAL AGENTS Chemical agents are grouped under several classifications. The broadest classification we will use is based on the general effect produced (i.e., severe casualty, harassment, or incapacitation). Within each general group, there are further breakdowns, the most convenient of which (from a medical point of view) is the classification by physiologic effect. Chemical agents may also be classified as lethal or nonlethal. Nonlethal agents will not kill you. Lethal agents are those that result in a 10 percent or greater death rate among casualties. They are further classified as persistent or nonpersistent, depending on the length of time they retain their effectiveness after dissemination. In the following paragraphs, we discuss the agents that produce the greatest number of fatalities and casualties among personnel who have been exposed to them. Nerve Agents Pharmacologically, the nerve agents are cholinesterase inhibitors (interfering with normal transmission of nerve impulses in the parasympathetic autonomic nervous system). Their reaction with cholinesterase tends to be irreversible, and reaction time varies with the agent. SIGNS AND SYMPTOMS OF EXPOSURE.- Nerve-agent intoxication can be readily identified by its characteristic signs and symptoms. If a vapor style="mso-spacerun: yes"> exposure has occurred, the pupils will constrict, usually to a pinpoint. If the exposure has been through the skin, there will be local muscular twitching where the agent was absorbed. Other symptoms will include rhinorrhea, dyspnea, diarrhea and vomiting, convulsions, hypersalivation, drowsiness, coma, and unconsciousness. TREATMENT.-Specific therapy for nerve agent casualties is atropine, an acetylcholine blocker. When exposed, each member of the Navy and Marine Corps is issued three 2 mg autoinjectors of atropine and three 600 mg autoinjectors of 2-PAM Cl. DO yes"> NOT give nerve agent antidotes for preventive purposes before contemplated exposure to a nerve agent. The atropine autoinjector consists of a hard plastic tube containing 2 mg (0.7 ml) of atropine in solution for intramuscular injection. It has a pressure-activated coiled-spring mechanism that triggers the needle for injection of the antidote solution. These injectors are designed to be used by individuals on themselves when symptoms appear. For medical personnel, the required therapy is to continue to administer atropine at 15-minute intervals until a mild atropinization occurs. This can be noted by tachycardia and a dry mouth. Atropine alone will not relieve any respiratory muscle failure. Prolonged artificial respiration may be necessary to sustain life. A second autoinjector containing oxime therapy (using pralidoxime chloride, or 2-PAMCl) can also be used for regeneration of the blocked cholinesterase. Since 2-PAMCl is contained in the kit of autoinjectors, additional oxime therapy is not generally medically recommended for those who have already received treatment by autoinjection. The 2-PAM Cl autoinjector is a hard plastic tube that, when activated, dispenses 600 mg of 2-PAM Cl (300 mg/ml) solution. It also has a pressure-activated coiled-spring mechanism identical to that in the atropine autoinjector. Self-Aid.-If you experience the mild symptoms of nerve-agent poisoning, you should IMMEDIATELY hold your breath and put on your protective mask. Then, administer one set of (atropine and 2-PAM Cl) injections into your lateral thigh muscle or buttocks, as illustrated in figures 8-4 and 8-5. Position the needle end of the atropine injector against the injection site and apply firm, even pressure (not jabbing motion) to the injector until it pushes the needle into your thigh (or buttocks). Make sure you do not hit any buttons or other objects. Using a jabbing motion may result in an improper injection or injury to the thigh or buttocks. Hold the atropine injector firmly in place for at least 10 seconds. The seconds can be estimated by counting "one thousand one, one thousand two," and so forth. Firm pressure automatically triggers the coiled mechanism and plunges the needle through the clothing into the muscle and at the same time injects the atropine antidote into the muscle tissue. Next, inject yourself in the same manner with the 2-PAM Cl injector, using the same procedure as you did for the atropine. This will now complete one set of nerve-agent antidotes. Attach the used injectors to your clothing (fig. 8-6) (to indicate the number of injections you have already received). After administering the first set of injections, wait 10 to 15 minutes (since it takes that long for the antidote to take effect) before administering a second set, if needed. If the symptoms have not disappeared within 10 to 15 minutes, give yourself the second set of injections. If the symptoms still persist after an additional 15 minutes, a third set of injections may be given by nonmedical personnel. After administering each set of injections, you should decontaminate your skin, if necessary, and put on any remaining protective clothing. Figure 8-4.-Thigh injection site.
Figure 8-5.-Buttocks injection site. Mark the casualty, if necessary. Do not fasten the hood. Administer, in rapid succession, three sets of the nerve-agent antidotes. Follow the procedures for administration as described previously in the self-aid section. NOTE: Use the casualty's own autoinjectors when providing aid. Do not use your injectors on a casualty. If you do, you may not have any antidote available when needed for self-aid. |
 |
|
|
||