Custom Search
|
|
 
|
||
|
PERIAPICAL ABSCESS A periapical abscess results when the pulp has become inflamed and a small pus-like abscess forms in the pulpal canal. If left untreated, the inflammation spreads out through the apex of the root and into the bone. As the abscess gets bigger, pressure from the inflammation and pus at the apex of the root may cause the tooth to be pushed up higher in its socket. The patient may complain the tooth feels "high" when biting and very sensitive to touch. Bone loss around the apex of the tooth can occur if left untreated. The abscess and bone loss at the apex cause a radiolucency appearing like a "grape" when viewed radiographically. The course that the abscess of pus follows from the apex, into the jaw bone, and drains into the mouth is referred to as a fistula NECROSIS The death of tissue is called necrosis. Pulpal necrosis can occur as a result of untreated pulpitis or from a traumatic injury. A tooth that is necrotic must be treated. The dead pulpal tissue will decompose, producing toxins that will smell foul or rotten when the tooth is being treated. Dental pain may or may not occur from a necrosis. PATHOLOGY OF THE PERIODONTIUM Periodontal disease is the most prevalent chronic disease of mankind. The term periodontal disease refers to all diseases of the periodontium and can affect the tissues around and supporting the teeth. As a basic dental assistant, you should know symptoms of periodontal disease your patients might describe: Bleeding gingival tissue during toothbrushing Tender or red swollen gums Receeding gingival tissue Tooth shifting or elongation (looks longer) Mobile (loose) teeth Purulent exudate (pus) in-between the teeth and gums Abnormal change in the fit of partial dentures Halitosis (bad breath) GINGIVITIS Gingivitis is an inflammation involving the gingival tissues. Conditions pertaining to the gingiva of principal concern to the Dental Assistant are marginal gingivitis and acute necrotizing ulcerative gingivitis. Marginal Gingivitis Marginal gingivitis (fig. 5-7) is the most common type of gingival disease. Most frequently it is the result of poor oral hygiene and affects both the gingival margins and papilla. Chief irritants are food debris and plaque around the necks of the teeth, interproximal spaces, or overhanging margins of dental restorations. Occasionally, a localized inflamed condition may exist from a popcorn husk or toothbrush bristle. Early formation of calculus deposits can also form under the gingival sulcus (subgingival) on the facial and lingual surfaces of the upper and lower teeth. Calculus deposits can also be responsible for the occurrence of marginal gingivitis, and if left untreated, may proceed to destruction of the supporting structures (as in periodontitis). Marginal gingivitis usually starts at the tips of the papillae and then extends to the gingival margins. Swelling, loss of stippling (orange peel texture of surface) of the attached gingiva, redness, easily retractable sulcus, and foremost, a tendency to bleed easily, are the main characteristics. This condition may be generalized (exist around all teeth), or it may be localized to one or two or a group of teeth. Acute Necrotizing Ulcerative Gingivitis Acute necrotizing ulcerative gingivitis (ANUG) (fig. 5-8) is a disease commonly referred to as trenchmouth, or Vincent's infection. It is characterized during the acute stage by redness, swelling, pain, accumulation of calculus around the sulcus of the teeth, and bleeding of the gingival tissues. Usually there is a film of necrotic white or grayish tissue around the teeth. This membrane may be wiped off, leaving a raw, bleeding base. The ulceration of the gingival crest results in a characteristic punched-out appearance and loss of the interdental papillae. There is an unpleasant odor and a foul taste in the mouth. The gingival tissues bleed easily when touched, and patients will complain of not being able to brush their teeth or chew well because of the pain or discomfort. PERIODONTITIS Periodontitis (fig. 5-9) is a chronic inflammatory condition that involves the gingiva, crest of the alveolar bone, and periodontal membrane. This condition results in loss of bone that supports the teeth, periodontal pocket formation, and tooth mobility. It usually develops as a result of untreated chronic marginal gingivitis. The color of the gingival tissues is intensified and becomes bluish red as the disease progresses. A gradual recession of the periodontal tissue will occur. Neglected deposits of calculus and formation of additional calculus over time contribute to the spread of the disease. Like marginal gingivitis, it may affect the entire dentition, or only localized areas.
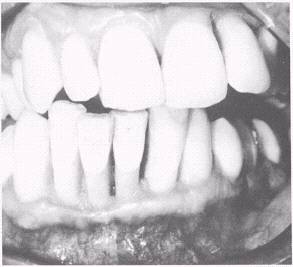
Figure 5-7.\Marginal gingivitis.
Figure 5-8.\Acute necrotizing ulcerative gingivitis (ANUG).
Figure 5-9.\Periodontitis. Pocket Formation As the inflammation continues, micro-organisms and their products progress toward the apex of the tooth, forming a pocket in which additional calculus forms. Frequently, the gingival margin also recedes toward the apex and the pocket is shallow. With pocket formation, the gingival tissue bleeds easily, and shelflike projections of calculus form between the teeth. These calculus formations irritate the interdental papillae, which become ulcerated and finally are destroyed. As the rest of the alveolar bone is resorbed, the attachment fibers of the periodontal membrane are loosened. They may remain attached to the tooth for a time, but finally they are destroyed, and the pocket can extend farther toward the apex of the tooth. Eventually, if the condition remains untreated, the tooth will be lost through destruction of its supporting tissues. Periodontal Abscess A periodontal abscess (fig. 5-10) usually results from long-continued irritation by food debris, plaque, deep deposits of calculus, or foreign objects such as a toothbrush bristle or popcorn husk being tightly packed in the interproximal spaces or within the walls of a pocket. The gingiva surrounding the area becomes inflamed and swollen. |
 |
|
|
||